Photobiomodulation research is conducted in dose. Consumer devices are operated by time.
Open almost any PBM paper and you’ll find a carefully reported protocol: wavelength, irradiance, treatment frequency, and delivered dose in J/cm². Dose is the controlled variable. It’s what researchers hold constant across subjects and what allows other groups to reproduce the work. If a study reports a positive outcome at 8 J/cm² using 660 nm light, dose is the parameter another researcher would need to reproduce that result.
Consumer devices rarely expose dose directly. Instead, they offer timers, distance recommendations, and mode selectors. Without fixed geometry and calibrated output, however, users have no practical way to know how many joules per square centimeter they are actually receiving.
The Guidance Problem
The obvious answer—”use X J/cm² for condition Y”—isn’t as straightforward as it sounds. Individual studies may report positive outcomes at a specific dose, but translating those findings into recommendations introduces both scientific and regulatory challenges.
More importantly, the literature rarely provides a single universally accepted dose. Different studies often use different wavelengths, treatment schedules, and energy densities.
What the Literature Actually Offers
Looking through the literature reveals a consistent pattern. Researchers typically report not only the wavelength used, but also the delivered dose.
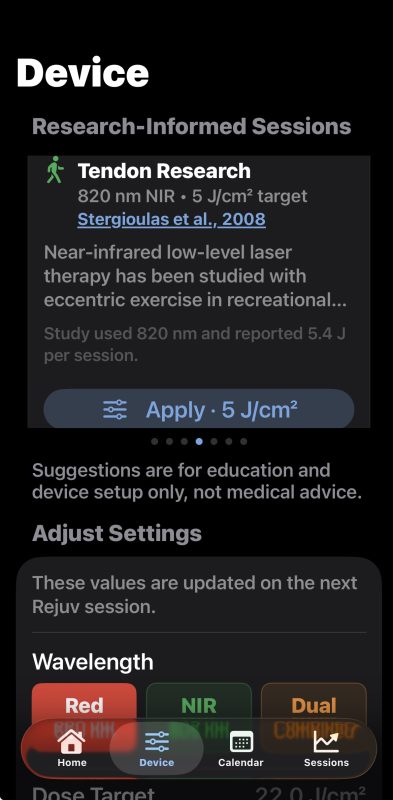
Wunsch and Matuschka (2014) examined skin appearance and collagen density using 660 nm light. Mota et al. (2023) studied wrinkle volume using 660 nm and 590 nm wavelengths with 3.8 J/cm² delivered. Kasowanjete et al. (2023) investigated wound-healing models using approximately 5 J/cm² delivered at 660 nm. Stergioulas et al. (2008) studied low-level laser therapy in the treatment of chronic achilles tendinopathy applying 5.4 J with 60 mW/cm² at 820nm.
The important observation is not that these studies agree on a single “correct” dose. Rather, they report the parameters that were actually studied. What the research offers, in other words, is not a recommendation but a record.
The Design Solution
Rejuv was designed to address the delivery side of this problem through fixed contact geometry, unit-level calibration, and closed-loop optical monitoring. If a user selects a dose target, the device can actually deliver it.
The feature that emerged from this is called Research-Informed Sessions, a set of cards that appear at the top of the Device configuration screen, before the manual adjustment controls.
Each card identifies an application area, the wavelength and dose range studied in the literature, a plain-language description of what was examined, a direct link to the primary source on PubMed, and a one-tap button that applies those settings to the device.
The card for skin health reads:
“Red light has been studied in controlled trials for skin appearance and collagen density.”
It links to Wunsch & Matuschka (2014) and configures the device to deliver 9 J/cm² in Red mode.
The card does not say the device will improve skin appearance. It does not say the user should expect any particular outcome. It says this is what researchers studied, at this dose, and here is the paper. The user makes their own decision.
The disclaimer below the card section is explicit: suggestions are for education and device setup only, not medical advice.
Why the Citation Link Matters
Linking directly to the primary source rather than summarizing it is a deliberate choice. It respects the user’s ability to evaluate evidence, it makes the basis for the suggestion transparent, and it places the supporting evidence in the literature rather than in the product.
A user who follows that link and reads the abstract will find a real study with real parameters. They’ll see that the dose the app suggested matches what the researchers used. The goal is not to prescribe treatment, but to ensure that when a user chooses a literature-based setting, the device can reproduce the protocol that was actually studied.
What This Feature Actually Does
Research-informed sessions do not tell users what outcomes to expect. They do something more modest: they connect a calibrated device setting to a documented research protocol.
For a field where studies are reported in dose but consumer devices are typically operated by time, that connection has historically been missing.
Rejuv was designed to make that connection visible.
The Rejuvulite companion app is available on TestFlight.